January 7, 2026
Birth Matters: How Labor and Delivery Shape Your Baby’s Feeding Journey

This is part one of an ongoing series on the many factors shaping your breast and chest-feeding journey. As a postpartum doula, I work with families every day who are doing everything “right” and still struggling — and most of the time, the reasons why are bigger than latch technique or milk supply. This series exists to help you zoom out, understand the full picture, and feel less alone in it. Part two will cover physiological factors and their effects on feeding. Stay tuned.
Here’s something that doesn’t get talked about enough: how your baby is born directly affects how feeding goes in those first hours, days, and weeks. As a lactation professional, one of the first things I want to know is your birth story — not out of curiosity, but because it gives me critical context for understanding what your baby might be working through.
The higher the level of intervention during birth, the more likely feeding challenges will appear right away. Sometimes, when feeding is significantly affected, babies need temporary alternative feeding methods — such as a nasogastric (NG) tube, cup feeding, spoon feeding, syringe feeding, nipple shields, supplemental nursing system (SNS), donor milk, or formula — while things get sorted out. In this post, we’ll walk through the birth factors that can affect breast and chest feeding, so you can start to connect those dots, too.
My biggest takeaway from diving into this topic is that the birth story is a clinical tool. I used to think of it as context — now I think of it as a roadmap. When a baby is struggling to latch, the answer is often written in how they arrived.
How Your Baby Was Positioned: Presentation Explained
“Presentation” is the clinical word for which part of your baby’s body is leading the way at the cervix — essentially, what part is going to come out first.
One thing worth knowing: all positioning terminology is described from your perspective as the birthing person. So if your care team says the baby is facing “left,” they mean your left.
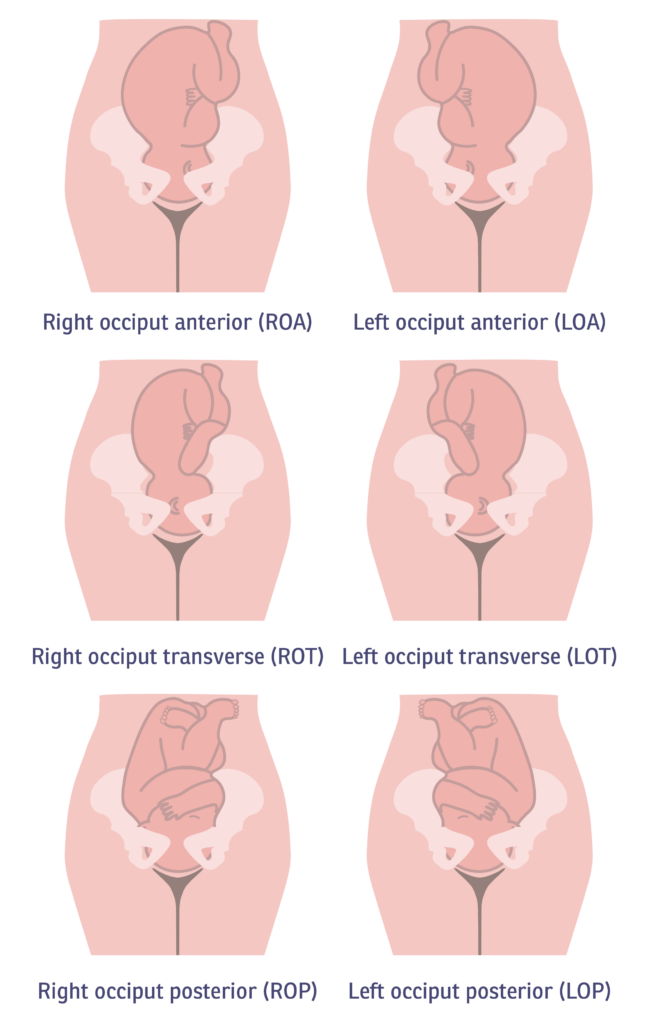
What Does “Occiput” Mean?
Occiput just means the back of your baby’s head. You’ll hear this word a lot in relation to positioning:
- Occiput Anterior (OA): Baby is face-down, with the back of their head toward your belly button. This is the most favorable position for labor.
- Occiput Posterior (OP): The back of the baby’s head is toward your spine — this is what people mean when they say a baby is “sunny-side up.”
Types of Presentation
Cephalic (Head-First) Presentations
Most babies arrive head-first, and there are several variations:
- OA: Back of head toward your front — the ideal position
- ROA / LOA: Back of head angled toward your right or left front
- ROP / LOP: Back of head angled toward your right or left back — these posterior positions are associated with longer, harder labors, which can lead to the mechanical interventions we’ll cover below
Complicated Presentations
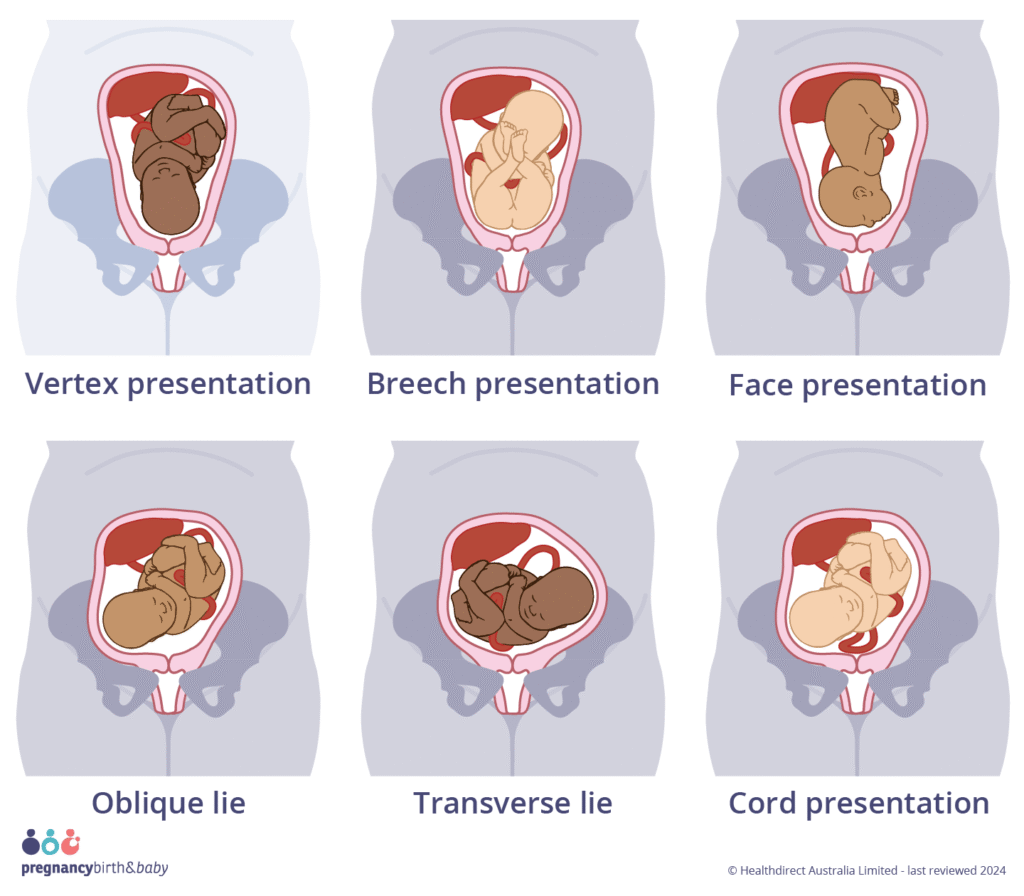
These involve a different body part leading the way, or a position that requires extra clinical management. They increase the likelihood of mechanical or surgical intervention — and with that, a higher chance of feeding challenges after birth.
- Face/Facial Presentation: The baby’s face is the presenting part at the cervix. This can result in bruising and swelling around the face and may affect the cranial nerves involved in feeding.
- Retroflexion: Premature flexion inside the uterus. It can result in a very complicated labor (back labor pain) and delivery management scenario. And it can also create complications for the fetus and infant after birth. This can lead to latching and attachment being affected, especially with a NICU stay, which may be necessary when retroflexion is involved.
- Breech Variations: Including frank breech (legs up by the face) and footling breech (one or both feet leading). These are incompatible with a typical vaginal birth and typically require mechanical or surgical intervention. Afterward, babies may experience bruising, swelling, muscular tension, or other challenges that affect feeding.
- Transverse: Baby is lying horizontally in the uterus — also incompatible with vaginal birth.
- Nuchal Cord: The umbilical cord is wrapped 360° around the baby’s neck. It can be tight or loose, and while it’s not always an emergency, it can cause muscular tension or torticollis (neck tightness), which we watch closely — we want babies to be able to turn their heads freely and comfortably in both directions.
- Nuchal Limb: An arm or leg wrapped around the neck. Similar to a nuchal cord, this can result in muscular tightness that makes latching harder — often more noticeable on one side.
- Placenta Previa: The placenta is positioned at the cervical opening ahead of the baby. This is always an emergency requiring cesarean delivery. Beyond the delivery itself, it can affect important early reflexes — like the tonic labyrinthine reflex — and instinctual processes like the breast crawl and baby-led latching.
Mechanical Interventions: What They Are and Why They Matter for Feeding
Mechanical interventions are tools or techniques used during labor and delivery to help move things along — whether that’s getting labor started, preparing the cervix, or safely delivering a baby who needs extra help. They’ve saved countless lives, and sometimes they’re absolutely necessary. But they can also affect both the birthing parent and baby in ways that show up in feeding afterward.
When I’m supporting a family postpartum, and I know there was a vacuum or forceps delivery, I’m already watching for signs of discomfort, tension on one side, or a baby who seems too sleepy to feed well. That context shapes everything about how I show up for them.
Vacuum-Assisted Delivery

The vacuum is one of the oldest birth tools we have, and it’s helped hundreds of thousands of babies arrive safely. A soft cup is placed on the baby’s head to provide gentle traction during pushing.
The risks to watch for: swelling, bruising, superficial scalp wounds, and — less commonly — bleeding inside the skull. Swelling and bruising can raise bilirubin levels, increasing jaundice. Jaundiced babies tend to be very sleepy, which makes feeding harder. And here’s the important irony: feeding is especially critical when a baby is jaundiced, because using the digestive tract (peeing and pooping) is the main way the body clears excess bilirubin.
Swelling near the surface of the head can also put pressure on cranial nerves — the nerves responsible for rooting, sucking, and swallowing. This can reduce sensation in the face and mouth, affecting the baby’s ability to sense and coordinate feeding movements. It can also affect their proprioception — their body’s sense of where it is in space — which matters more than you might think when a tiny human is learning to latch.
Forceps
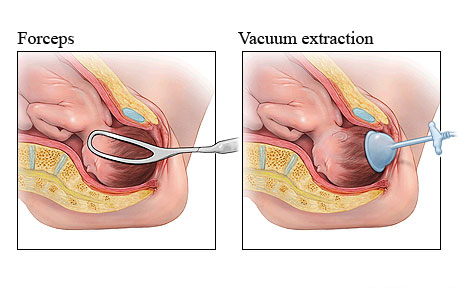
Forceps have also been around for a very long time, and many people comment that they look like salad tongs! They’re used to help guide the baby’s head through the birth canal when extra traction is needed.
Forceps have been very helpful for the person mediating childbirth, such as an OBGYN or a midwife, to gain better traction on the infant’s head, which can sometimes assist when the infant is stuck in the birth canal, likely due to one of those complicated presentations mentioned before.
They can also put significant traction on the cervical spine. Luckily, babies have extra fluid in those spinal discs, which significantly protects the infant, and that’s why forceps can be used at all.
However, it can cause bruising of the skull and face, and it does carry an increased risk of cranial fracture because of the pressure that the forceps put on the cranial bones, even though they’re very tough bones, and they’re very mobile for good reason, the fracture of a cranial bone can cause swelling, bleeding and signicant pain to the infant.
There are also increased risks of long-term complications such as cerebral palsy (CP). And this can affect the infant’s feeding due to temporary differences in muscle tone, either from swelling or from a fractured cranial bone. Or we can see facial ballsy from impacting the cranial nerves or compression of the cranial nerves.
We can see significant infant discomfort from bruising or fractures, and we can see a NICU stay that may require temporary separation from the infant to their parent, leading to more infant feeding challenges along the line and different methods of feeding to nourish your baby.
Internal Fetal Monitoring
This is a less-intensive mechanical intervention that is more recently available. While generally safe, the internal fetal monitoring has a superficial risk of damage to the fetal scalp and an increased risk of infection, which can cause the baby to be sleepy or to feed less. This risk to the infant also includes temporary separation due to a NICU stay because of that infection. Or the administration of antibiotics as a precaution during labor. The administration of antibiotics can also affect the infant’s gut flora.
Amnioinfusion
When the amniotic fluid levels get too low during labor — often because the water broke a long time ago — the care team may reinfuse fluid into the amniotic sac. This is usually done to protect the baby by preventing cord compression (which can cut off blood flow and oxygen).
The risks include umbilical cord prolapse (the cord slipping out ahead of the baby and being compressed as the baby descends), slowed fetal heart rate, and, in rare cases, uterine overstretching. Like many of the interventions here, it can also result in a NICU stay, delayed initiation of feeding, and temporary separation — all of which affect the feeding relationship.
Surgical Interventions: C-Section Birth and Feeding
Cesarean birth deserves its own conversation here because it’s so common and so often left out of feeding discussions.
A cesarean is major abdominal surgery, and the recovery alone can affect how quickly and comfortably you’re able to hold, position, and feed your baby. But beyond the physical recovery, there are a few specific ways C-sections can influence early feeding:
- Delayed skin-to-skin contact: In many hospital settings, immediate skin-to-skin after a cesarean isn’t always offered or prioritized — though it absolutely can be with the right advocacy and support. That early contact matters for feeding initiation.
- Anesthesia and medication: The medications used during and after surgery can affect both your alertness and your baby’s in those first hours.
- Hormonal differences: Labor itself triggers a hormonal cascade that helps initiate milk production. When labor doesn’t happen — or is cut short — that process can be delayed, which sometimes means milk takes a little longer to come in. This is common and manageable, but worth knowing in advance.
- Baby’s lungs and alertness: Babies born via cesarean, especially before labor begins, miss the compression of the birth canal that helps clear fluid from their lungs. This can make them a little gurglier or sleepier in the early hours, which can affect feeding.
None of this means feeding won’t work; it absolutely can and does. It just means the starting line looks a little different, and having support in place early makes a real difference.
Genetic and Congenital Conditions That Affect Feeding
Sometimes, feeding challenges aren’t rooted in how birth went — they’re connected to conditions the baby was born with. We also have other defects that can cause feeding difficulties. These are things the baby is born with that can impact their early function, development, anatomy, physiology, and early feeding. These genetic and congenital defects can pose significant challenges for the lactation provider and the parent who wants to breast or chest feed. Here are some disorders or defects that we may encounter as a lactation provider or parent:
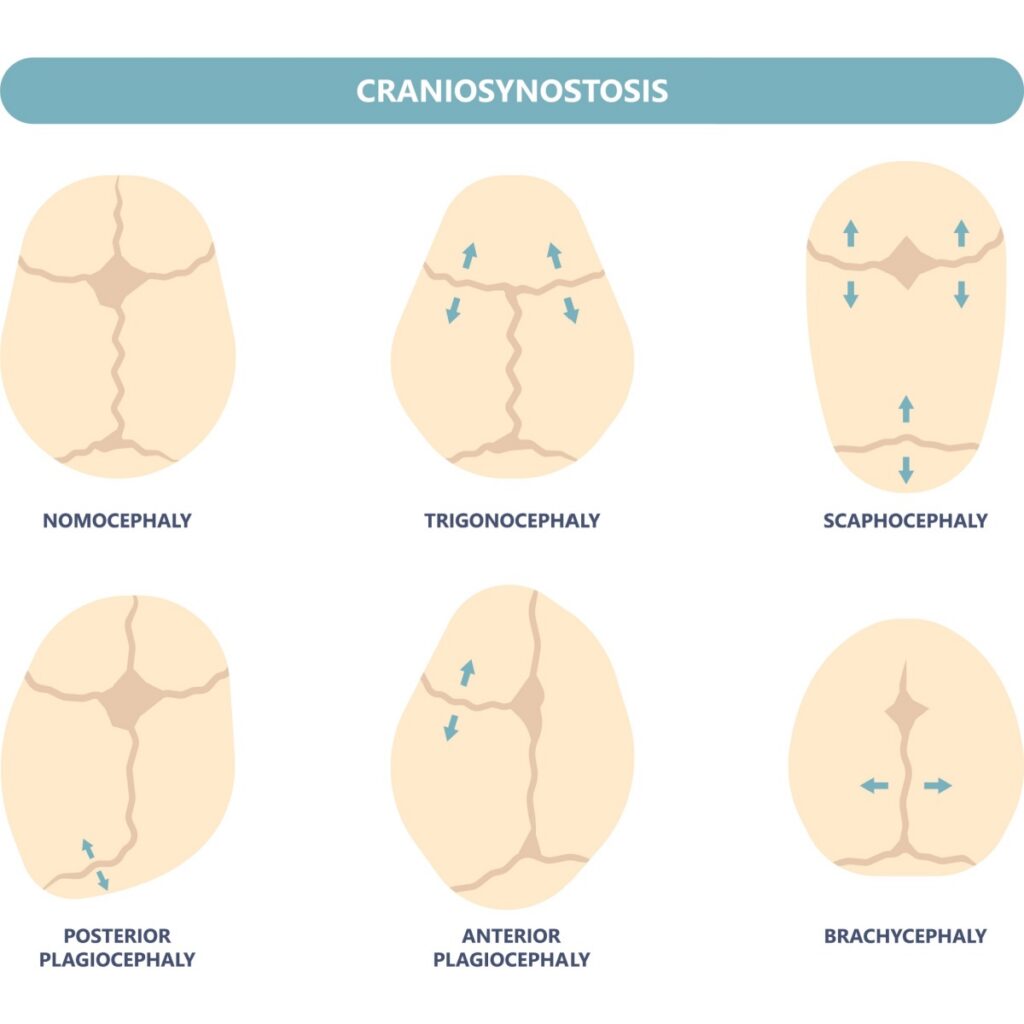
Cephalic (Skull) Disorders
These involve the bones of the skull fusing too early — before the brain has finished growing. When the skull can’t flex and reshape normally, it can affect the internal pressure changes that happen during feeding (babies create a vacuum to draw milk, and skull flexibility plays a role in that). It can also require surgical or mechanical intervention during delivery, adding another layer of feeding challenge.
Examples include: Trigonocephaly (triangular skull), Scaphocephaly, Brachycephaly, and Synostotic Plagiocephaly (a flat spot on one side of the skull).
Midline Defects
During early fetal development, the midline is like the body’s central scaffolding — it’s what allows the body to form symmetrically. Defects along this line can affect anatomy and function in a wide range of ways.
Midline defects include: cleft lip or palate (hard or soft palate, one or both sides), lip/cheek/tongue ties, certain heart defects, esophageal defects, diaphragmatic defects, and neural tube defects like spina bifida. All of these can bring with them some combination of pain, fatigue, and structural challenges that make breast and chest feeding harder — though not always impossible.
Cleft Lip and Palate: A Closer Look
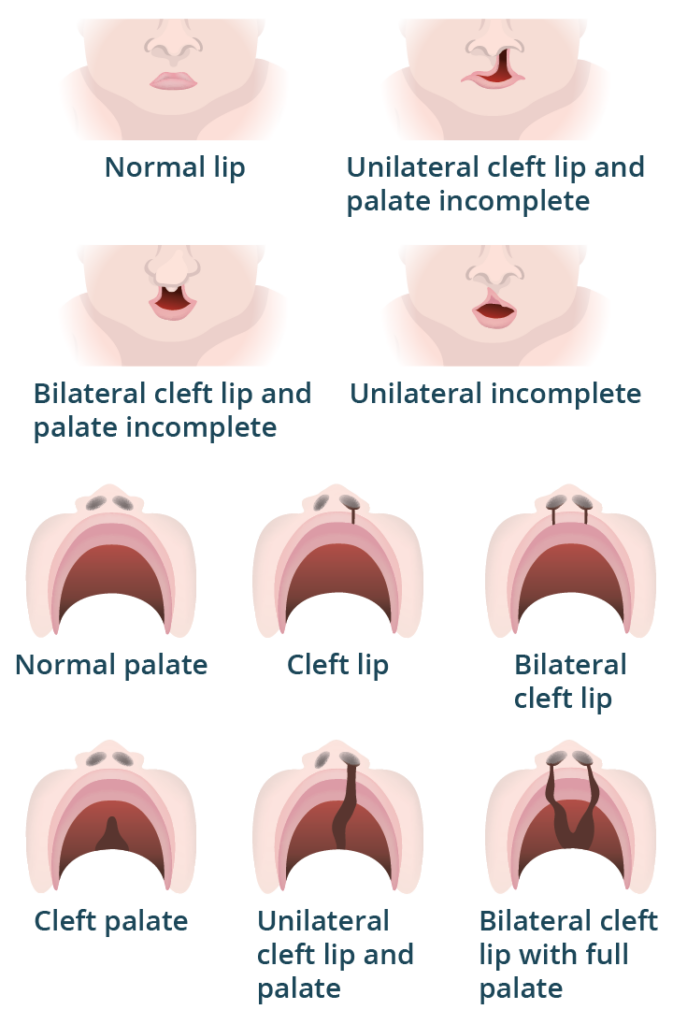
Clefts vary enormously — from a small notch in the lip to a complete opening through both the lip and the roof of the mouth, on one or both sides. The key issue for feeding is suction: babies need to create a vacuum to draw milk from the breast or chest. With a significant cleft — especially one involving both the lip and palate — creating that vacuum may not be possible without adaptive tools or techniques.
This doesn’t mean feeding is off the table, but it does mean we need to think creatively and get the right support in place early.
Growth and Metabolic Disorders
These disorders affect the infant’s growth and metabolism, require different feeding needs, and can be very medically complex. These can affect how the infant needs to feed because the infant’s metabolism is the rate at which the infant burns calories to support basic systemic processes and functions (the infant may need to eat more frequently or consume more calories to keep up with energy demands). We may have more complex nutritional needs in these babies than in average babies.
In some cases, such as galactosemia, direct breastfeeding or the use of human milk is contraindicated until interventions can be made.
The most common and most serious of these growth and metabolic disorders are included in the standard newborn screening in the United States. This means that the baby’s blood is taken early on, then the screening is repeated to rule out the most common growth and metabolic disorders.
Neurological Conditions
The cranial nerves — numbered I through XII — are responsible for the reflexive processes that make feeding possible: rooting, sucking, swallowing, and more. If any of these nerves are compromised (by birth trauma, a congenital condition, or something else), it can disrupt feeding in a number of ways.
Low muscle tone is a common example: if a baby can’t sustain the muscle effort required to feed effectively, they may tire out before getting enough milk. This makes breast and chest feeding more complex — but not necessarily impossible- and additional feeding support can make a significant difference.
A Note for Parents
Birth is hard! And feeding after a complicated birth can be even harder. So much has to align for breastfeeding or chest feeding to go smoothly from the start, and many of the factors that shape that experience are completely out of your hands.
If your baby was born with the help of any intervention, or spent time in the NICU, you may already be navigating the ripple effects — the separation, the stress on your baby’s body, the interrupted early hours that you can’t get back. That is a real loss, and it matters.
What I want you to hear most is this: if feeding isn’t going the way you hoped, it is not because you didn’t try hard enough. The path from birth to a smooth feeding relationship is long, and there are many places along the way where things can get complicated — none of which are your fault.
Please don’t go into it alone. A lactation professional can look at your whole picture. Your birth story, your baby’s patterns, and your goals can help you figure out what’s actually going on and what your real options are. You deserve that support. Here’s how I’d say this to a parent sitting across from me:
“Birth is hard, and your baby felt every bit of it, too. That doesn’t mean something went wrong, it means your bodies worked incredibly hard together, and sometimes that leaves a mark that needs a little extra attention.”
Everything in this post points back to something I believe deeply — feeding isn’t just about latch technique or milk supply. It’s about the whole story: the birth, the baby’s nervous system, the parents’ experience, and the relationship being built in real time. That’s why a holistic, baby-led lens isn’t a luxury. It’s the only way to actually help.
Part Two is coming, diving into physiological factors and how they affect breast and chest feeding. Stay tuned.
Resources
Haden, Bryna. (2026). Impacts of Gestation and Birth.https://www.goldlearning.com/speaker/746/bryna-hayden. Gold Lactaction Academy. Accessed January 03, 2026.
Sakalidis VS, Williams TM, Hepworth AR, Garbin CP. Hartmann PE, Paech MJ, Al- Tamimi Y, Geddes DT. A comparison of early sucking dynamics during breastfeeding after cesarean section and vaginal birth. Breastfeed Med. https://pubmed.ncbi.nlm.nih.gov/22845858/2013 Feb;8(1):79-85. doi:
10.1089/bfm.2012.0018. Epub 2012 Jul 30. PMID: 22845858
Smith LJ. Impact of birthing practices on the breastfeeding dyad. J Midwifery Womens Health. 2007 Nov-Dec:52(6):621-30. https://pubmed.ncbi.nlm.nih.gov/17984000/ doi: 10.1016/j.jmwh.2007.07.019. PMID: 17984000
Bruns DA, CampbellE. Twenty-five additional cases of trisomy 9 mosaic: Birth information, medical conditions, and developmental status. Am J Med Genet A. 2015 May;167A(5):997-doi: 10.1002/ajmg.a. 36977. Epub 2015 Mar 8. https://pubmed.ncbi.nlm.nih.gov/25755087/ PMID: 25755087.
Javier A, Farlow B, Barrington KJ. Parental hopes, interventions, and survival of neonates with trisomy 13 and trisomy 18. Am J Med Genet C Semin Med Genet. 2016 Sep:172(3):279Javier A, Farlow B, Barrington KJ. Parental hopes, interventions, and survival of neonates with trisomy 13 and trisomy 18. Am J Med Genet C Semin Med Genet. 2016 Sep:172(3):279-doi: 10.1002/ajmg.c.31526. Epub 2016 Aug 23. https://pubmed.ncbi.nlm.nih.gov/27550159/ PMID: 27550159
Mercuri E, Pera MC, Brogna C. Neonatal hypotonia and neuromuscular conditions. Handb Clin Neurol. 2019;162:435-448. doi: 10.1016/B978-0-444-64029-1.00021-7. https://pubmed.ncbi.nlm.nih.gov/31324324/ PMID: 31324324.
Stanley MA, Shepherd N, Duvall N, Jenkinson SB, Jalou HE, Givan DC, Steele GH, Davis C, Bull MJ, Watkins DU, Roper RJ. Clinical identification of feeding and swallowing disorders in 0-6 month old infants with Down syndrome. Am J Med Genet A. 2019 Feb:179(2):177-182. doi: 10.1002/ajmg.a.11. Epub 2018 Dec 27. PMID: 30588741; https://pmc.ncbi.nlm.nih.gov/articles/PMC6349541/ PMCID: PMC6349541
Leave a Reply

Get the Guide!
Put a brief description of what to expect here. Don't have a mailing list? Hide this section in one click!



")

Be the first to comment